By Blaise Dupont, Year 12
Mental health is one of the key aspects to our overall well-being, and easily one of the most riveting to discuss. A single miscalculation in the development of the brain can entirely alter the functioning of an individual. This can include their behaviour, language, sensory input, coordination, visual perception, etc. There are labels for these alterations to the functioning of the brain, and various categories that refer to the general areas of the brain which they affect. Personality disorders is one of those categories of psychological disorders that mainly affects the frontal lobe of the brain, thus a huge part of a person’s overall personality.
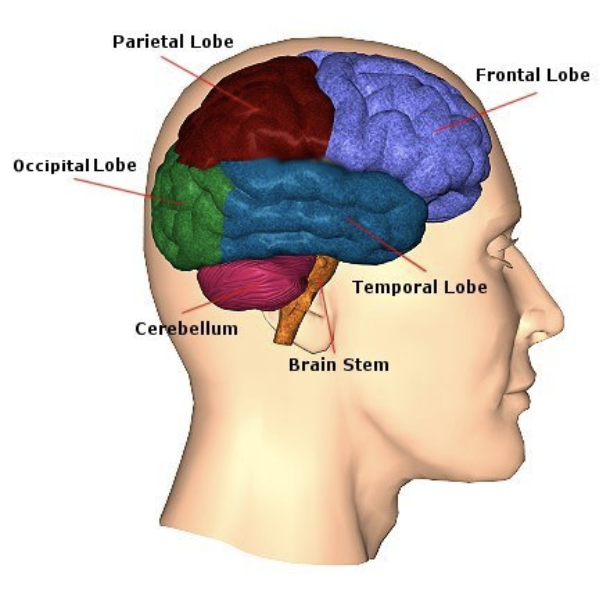
The human brain can be divided into several different sections, each having their own individual functions; these sections include the frontal lobe, the parietal lobe, the occipital lobe, the temporal lobe, the cerebellum and the brainstem. Despite being separate, these sections work in symbiosis and overlap in their abilities.
- The Frontal lobe:
- The frontal lobe is responsible for complex cognitive functions such as reasoning, organisation, calculating and even short-term memory. It also is responsible for voluntary movement and expression.
- The Parietal lobe:
- The parietal lobe allows for sensory perception and integration. It receives and processes sensory input including, sound, touch, smell, taste, and other sensory registries.
- The Occipital lobe:
- The occipital lobe is responsible for visual perception, both of colour and motion. It is also involved in visual interpretation and orientation.
- The Temporal lobe:
- The temporal lobe allows for auditory processing, along with emotional regulation and long-term memory. The temporal lobe is also key in processing language, and even visual perception.
- The Cerebellum:
- The cerebellum manages the overall balance of the body, its motor abilities and coordination. It calculates the movements of the body and muscles for smooth mobility.
- The Brainstem:
- The brainstem conducts diverse involuntary functions such as breathing, or heart rate. It also controls the very signals that the brain receives, as it resides at the intersection between brain material and the spinal cord.
As mentioned previously, personality disorders mainly affect the frontal lobe, however it can also affect other parts of the brain, typically the temporal lobe. This is generally due to issues in communication between the temporal and frontal lobes, either genetic disformations or issues raised in the development of the brain in childhood.
There are three different categories of personality disorders. These categories are called clusters and are divided as such: Cluster A – eccentric, Cluster B – dramatic, and Cluster C – anxious. Cluster A personalities are characterised by odd behaviours, often socially undesirable, with sceptical thinking patterns and superstitious ideologies. There are three variants of this personality cluster:
- Paranoid Personality Disorder(PPD) – This disorder is both chronic and lifelong, and is distinguished by pervasive patterns of paranoid thinking and suspicion. Individuals with this disorder struggle greatly to trust others, often anticipating only the worst out of others’ intentions. They tend to seek evidence in their surroundings to further prove their paranoid theories, making them hypersensitive, though often neglecting any alternate explanations.
- Subtypes include: expansive paranoia, fanatic, querulant, delusional
- Schizoid Personality Disorder(SPD) – This disorder is also both chronic and lifelong. SPD is often recognised by a significant lack of emotional range, particularly in expression. Individuals with this disorder have little interest in forming relationships with others and appear rather reserved. Due to their lack of emotional range, they tend to be extremely passive and unreactive on the surface, even towards important life events, or when provoked. They often form strong bonds with animals.
- Subtypes include: affectless, languid, remote, depersonalised
- Schizotypal Personality Disorder(STPD) – This disorder is lifelong and identified by odd social behaviours and habits. The disorder is typically paired with inappropriate affect, which causes an individual to not react appropriately to certain situations (e.g. laughing in rather upsetting, or sad situations), dissociation and perceptual illnesses. Individuals with this disorder are often socially isolated due to their general awkwardness with social interactions and often suffer social anxiety. They tend to hold unconventional beliefs and paranoid thinking patterns, making them prone to psychotic episodes.
- Subtypes include: perceptual aberration, magical idealism, revised social anhedonia, physical anhedonia
Cluster B personality disorders are described as dramatic. This is a reference to the general lack of emotional and chemical balance in the brain of individuals with these disorders. The lack of chemical balance in the brain allows these individuals to experience either extreme emotions, or dull emotions, but rarely an equilibrium of emotional stability. The four disorders under this cluster are:
- Antisocial Personality Disorder(ASPD) – This disorder is considered long-term, but symptoms tend to grow milder with age. It is often marked with pervasive deviant behaviour including destructive habits such as manipulation, deceptiveness, impulsivity, recklessness and addiction. Hypersexuality is also common in people with ASPD. Individuals with this disorder can often be irritable and thus aggressive, they can display callous, unemotional traits (informally known as psychopathy). This instability tends to lead to consequences, to which these individuals will most likely not take responsibility for, as they lack the ability to differentiate right from wrong, especially when it is to their advantage. As a result of these individuals’ general lack of empathy and remorse, it can be very difficult for them to maintain relationships, even ones that may be valuable to them, which can ultimately lead to great feelings of contempt and overwhelming emptiness/loneliness.
- Subtypes include: covetous, risk-taking, malevolent, tyrannical, malignant, disingenuous, explosive, abrasive
- Borderline Personality Disorder(BPD) – Similarly to ASPD, this disorder is also long-term as its symptoms tend to wear off with age. This disorder is often confused with BD, or bipolar disorder, for its extreme mood shifts, however it involves much more complex issues in the brain. In fact, as this disorder is mainly trauma-based, it is known for its intricacy and difficulty of treatment as every individual with this disorder tends to have varying undertones of other Cluster B personality disorders or callous-unemotional traits intertwined with their original psychology. This is due to the disorder often being a reflection of the trauma/abuse inflicted on the individuals’ new defence mechanism. This causes a great split in these individuals typically demonstrated in the form of unstable relationships, a distorted sense of self and performance of dangerous activities. These individuals may struggle greatly with their extreme emotions and regulation, making them more susceptible to addiction and self-harm. Those with BPD often struggle with hypersexuality as well, due to chemical imbalances in the brain. These individuals tend to experience feelings of detachment and emptiness, particularly when faced with their own fears of abandonment, which can be triggered by any particular situation, to which non-borderlines would consider normal. This can create significant feelings of isolation and loneliness as non-borderlines can hardly understand or relate to the severity of BPD episodes.
- Subtypes include: discouraged, impulsive, petulant, self-destructive(also known as quiet BPD)
- Histrionic Personality Disorder(HPD) – This disorder is lifelong, and quite distinct for its intense behaviours, particularly of attention-seeking variety, which includes seductive and overly provocative demonstrations. Individuals with this disorder will be in constant search for attention and will generally appear charmingly lively, vivacious, overly-enthusiastic and extroverted. They will crave constant stimulation, and due to their easily influenceable lifestyle, they will be more susceptible to destructive habits in order to gain validation from others. As a consequence of their thirst for attention, they tend to be egocentric, self-indulgent, fluctuant and even manipulative. They may perceive relationships to be closer than they really are and can be quickly disappointed when faced with reality. Despite their egocentric nature, individuals with HPD do not necessarily lack empathy for others, they simply struggle with forming deeper bonds with others, often masking with shallow emotions, as they deeply believe that they are constantly putting on a show for others. These individuals will depend on the validation of others in order to feel good about themselves, and will risk anything about themselves, including people they care about, to get the attention they crave, ultimately resulting in destructive behaviours. They may also struggle with romantic relationships as their impulsivity and fluctuating emotions make it difficult for them to maintain stable relationships.
- Subtypes include: appeasing, vivacious, tempestuous, disingenuous, theatrical, infantile varieties
- Narcissistic Personality Disorder(NPD) – This disorder is long-term, as its symptoms moderate with the years. NPD is defined by self-centred thinking patterns, with exaggerated feelings of self-importance and a thirst for attention, or “supply” (term used to describe an emotional reaction, or emotional energy given). Grandiosity is an important, and dangerous element of the narcissistic persona. It develops this delusional sense of status and power in which an individual truly and deeply believes that they are inherently special, or different from others, and fated for greatness. When faced with the realities in which the individual is not as powerful as they believed, it can cause great shame, particularly in narcissists. Narcissists feel great bounds of shame, typically referred to as a “narcissistic crash”, in which their ego is broken down, and their confidence is stripped away for some time. Individuals with this disorder often have a diminished ability to empathise with others, some may be capable of feeling empathy, but choose not to. This results in the manifestation of interpersonally exploitative behaviours, manipulating others into giving them the attention that they crave. In relationships, individuals with this disorder will have difficulty sharing emotions with their partner, even when the willingness is present. They are also prone to hypersexual behaviours due to chemical imbalances in the brain. Deep down, individuals with NPD, particularly self-aware individuals, will fear for the inevitable reality that they are not as special as they would like to be, and will crash, typically lashing out on others in hope of gaining back the control they feel they have lost.
- Subtypes include: overt, covert, communal, antagonistic, malignant
Cluster C personality disorders are commonly defined by anxious behaviours, and are unsurprisingly linked with anxiety. Individuals with these disorders experience acute levels of anxiety and struggle to live fulfilling lives out of fear. The three disorders under this cluster include:
- Avoidant Personality Disorder(AvPD) – This disorder is chronic and characterised by severe social anxiety and fear of interacting with others. This is due to these individuals experiencing overwhelming inhibition, feelings of inferiority and inadequacy. Despite craving intimacy, these individuals will avoid any possible contact with others, often inflicting self-isolation. They are incredibly sensitive to criticism and rejection, as they have gravely low self-esteem. They will appear timid, however on the inside they are hypersensitive to the world around them and will fear embarrassment, as they tend to be quite insecure of themselves.
- Subtypes include: phobic, conflicted, hypersensitive
- Dependent Personality Disorder(DPD) – This disorder is long-term and distinguished by pervasive psychological and physical reliance on others. These individuals will only commit to the bare minimum independently, as they live in constant unease with themselves. They cannot function properly without the assistance of others and will be in shambles if someone close to them leaves(eg. a partner). They rely on the approval of others and cannot stand to be in control of a situation, they tend to be helpless and severely submissive. Individuals with this disorder cannot trust themselves and will prioritise the needs of others over their own. This can lead to abusive relationships in the future where the individuals may be taken advantage of and suffer severe trauma.
- Subtypes include: passive-aggressive, counter-dependent
- Obsessive-Compulsive Personality Disorder(OCPD) – This disorder is long-term, and can become lifelong, and is defined by an obsession with rules, lists, schedules and order. These individuals will appear highly productive and self-sufficient, as they will often take on as much responsibility as possible, refusing to delegate responsibility to others due to their perfectionistic nature and neediness for control. They tend to be radical in their opinions and rather stubborn. These individuals have their own idea of reality, and are difficult to shift, they can be self-righteous. Often confused with OCD, this disorder has its distinctions. Unlike OCD, where an individual lives by impulsive compulsions to relieve their anxiety, individuals with OCPD are more reliant on perfectionism and detail, often having detrimental effects on their surroundings, they lack self-awareness. Whereas OCD resides as an anxiety disorder, OCPD takes on greater proportions in affecting an individual’s perception of their reality and themselves.
- Subtypes include: aggressive, pleasing
Moreover, there are other personality disorders which were not included in this list, as they do not make an official part of the DSM-5(Diagnostic and Statistical Manual of Mental Disorder, volume V). These “personality disorders” include: Depressive Personality Disorder, Cyclothymic Personality Disorder, Passive-Aggressive Personality Disorder, Masochistic Personality Disorder, Sadistic Personality Disorder, Psychopathy, Haltose Personality Disorder (disinhibited personality, or the unstable psychopath), Immature Personality, Organic Personality Disorder (cluster of trauma turned into various patterns of personality). These disorders are not officially classified as a diagnosis, they are instead attributed to similar mental disorders, such as Cluster B personality disorders(BPD, ASPD), Cluster C(DPD), or even mood disorders (cyclothymic is now recognized as BP type III, or rapid shifting BP).
The personality disorders discussed are often a result of childhood trauma and abuse. Individuals may grow up in an unhealthy environment and develop various defence mechanisms to counter the negative effects of the trauma they have endured. This can also come in the forms of other mental illnesses, as it is not limited to personality disorders. However, when it comes to abuse, personality disorders can be quite common in the altered development of the brain, as it attempts to build itself around the damage (plasticity).
In conclusion, it is always good to keep in mind that individuals living with these disorders have developed them for a number of reasons (result of psychological trauma, genetic predisposition, physical damage to the brain), and that it is crucial to remain open-minded about their issues. Proper communication and patience have proven to be very effective in allowing these individuals to heal, or at least to allay their symptoms. It is key that each individual is treated with respect and empathy, as their struggles can go unnoticed. Personality disorders, especially Cluster B disorders, often have a negative reputation for their manipulative behaviours. Therefore it is important to understand that not all of these individuals seek to harm others, and that for the most part, these individuals are only protecting themselves and are not always fully aware of the damage that they are causing. However, this does not mean that one should let themselves be taken advantage of, in hopes of another individual changing their destructive behaviours. One should always look after oneself first, before attending to the needs of others. This is particularly the case with mental health; while it is virtuous to be kind and patient, do not let your boundaries be crossed. Your own health should always be your priority.